
The Cognitive Burden Simulator: Ranking Task Item
6 ene 2026
UK
,
Spain
In this article, we examine the cognitive burden of a ranking-style COA item, a format that goes beyond simple selection or frequency judgement by requiring patients to make comparative decisions across multiple symptoms. The item is as follows:
“In the past month, which of the following symptoms have caused the most difficult in your daily life? Select up to three and rank them in order of impact (1 = most impact, 3 = least impact):
☑ Pain Rank: 1
☑ Fatigue Rank: 2
☐ Shortness of breath Rank: ___
☐ Difficulty concentrating Rank: ___
☐ Dizziness Rank: ___
☐ Muscle weakness Rank: ___
☑ Nausea Rank: 3
☐ Other (please specify: ___________) Rank: ___”
On the surface level, this looks straightforward. It is a familiar checklist with a ranking twist. However, in practice, it asks patients not only to recognise relevant symptoms but to prioritise and order them by subjective impact, layering comparative reasoning and metacognitive judgement on top of recognition and recall.
What Makes This Item Easy
Familiar concepts: symptoms like pain, fatigue, dizziness and nausea are everyday words, easily recognised by most patients.
Concrete timeframe: “In the past month” sets a clear recall window, avoiding the vagueness of terms like “recently”.
Limited selection set: Eight options is a more manageable list compared to a 15–20-word descriptor inventory.
Structure instruction: Patients are told to “select up to three and rank them”, which sets clear boundaries.
What Makes This Item Difficult
1. Dual task: selection + ranking
Patients must first scan the list and decide which symptoms apply.
Then they must compare those symptoms and order them by subjective impact.
This layering shifts from simple recognition into forced prioritisation, which is cognitively heavier.
2. Comparative reasoning
Unlike checklist items where multiple boxes can be ticked independently, ranking requires side-by-side evaluation.
Patients must weight severity, frequency and functional disruption across different symptom, such as pain versus fatigue versus cognitive issues.
3. Metacognitive demand
The item asks patients to step back and consider relative impact: “which symptom interferes most with my daily life?”
This requires integration of recall, subjective judgement and cross-domain comparison.
4. Working memory load
To answer, patients must hold in mind:
- The timeframe (past month).
- The instruction (select up to 3, rank them 1 to 3).
- The list of 8 symptoms.
- Their personal experience of each symptom.
- The comparative outcome (ranking and ordering).
- That’s 6-7 active concepts, before even writing down a response.
5. Other-specify option
The “Other (please specify)” field adds an open-text burden: patients must recall, formulate and write down a symptom in their own words, then integrate it into the ranking.
6. Translation and cultural issues
Terms like weakness, fatigue or difficulty concentrating may not map neatly other languages.
Cultural stigma around cognitive issues may alter whether patients select or rank certain symptoms at all.
CBS Breakdown Table
Level | Component Type | Text | Notes |
Root | Sentence | In the past month, which of the following symptoms have caused the most difficulty in your daily life? Select up to three and rank them in order of impact (1 = most impact, 3 = least impact). | Full item stem (two-part instruction) |
1 | Timeframe | In the past month | Anchors recall to ~30 days |
1 | Main Clause | Which of the following symptoms have caused the most difficulty in your daily life? | Core evaluative task |
2 | Construct | Symptoms | Domain of assessment |
2 | Qualifier | Most difficulty in your daily life | Requires subjective weighting across domains |
1 | Instruction | Select up to three and rank them in order of impact (1 = most impact, 3 = least impact) | Dual task: selection + ranking |
1 | Response Options | Pain, Fatigue, Shortness of breath, Difficulty concentrating, Dizziness, Muscle weakness, Nausea, Other (please specify) | Recognition set (8 options) |
2 | Symptom 1 | Pain | Physical |
2 | Symptom 2 | Fatigue | Physical/functional |
2 | Symptom 3 | Shortness of breath | Physical |
2 | Symptom 4 | Difficulty concentrating | Cognitive |
2 | Symptom 5 | Dizziness | Neurological/functional |
2 | Symptom 6 | Muscle weakness | Physical |
2 | Symptom 7 | Nausea | Somatic |
2 | Symptom 8 | Other (please specify: ________) | Open-ended; additional recall and writing burden |
Visual Map Structure and Diagram
The MindMap Structure
Circle | Burden Layer | Patient’s Inner Thought Simulation |
0 – CBS Core (Parsing) | Sentence parsing | “Okay, timeframe = past month. Task = pick symptoms. Instruction = choose up to three AND rank them 1–3.” |
1 – WM Limits | Capacity strain | “I need to hold the stem (past month, daily life impact, up to 3, rank 1–3) AND the list of symptoms in my head while I decide. That’s already 5–6 chunks.” |
2 – Visual Processing | Layout, scanning | “Let me scan down the list — Pain, Fatigue, Shortness of breath… Which ones apply? I need to make sure I don’t skip a line or put the wrong number in the wrong box.” |
3 – Linguistic / Cultural | Interpretation of terms | “Does ‘difficulty concentrating’ mean at work? Or just when reading? Is ‘muscle weakness’ the same as tiredness? What exactly counts as ‘nausea’ versus dizziness?” |
4 – Delivery Mechanism | Paper vs. digital | “On paper I have to write numbers in the boxes. On a screen, I might drag-and-drop or click — easier, but I still need to double-check.” |
5 – Contextual Stressors | Patient condition | “I’m already exhausted. Thinking about this makes me feel worse. Ranking them feels like a test of which problem is ‘worst.’” |
6 – Wording Ambiguity | Instruction clarity | “‘Up to three’ — so if I have four main symptoms, which do I leave out? And what if one fluctuates? Should I still rank it?” |
7 – Presentation Conventions | Scale/jargon conventions | “I’m used to ticking boxes, but now I have to number them. Do I put a ‘1’ inside the box or next to it? What if I mis-rank?” |
8 – Emotional Salience | Discomfort, stigma | “Admitting fatigue feels like admitting weakness. And if I put ‘pain’ first, will the doctor think I’m complaining too much?” |
9 – Overload / Collapse | Coping heuristics | “This is too much. I’ll just pick the three most obvious ones and assign 1–2–3 quickly, even if it doesn’t reflect the nuance of my experience.” |
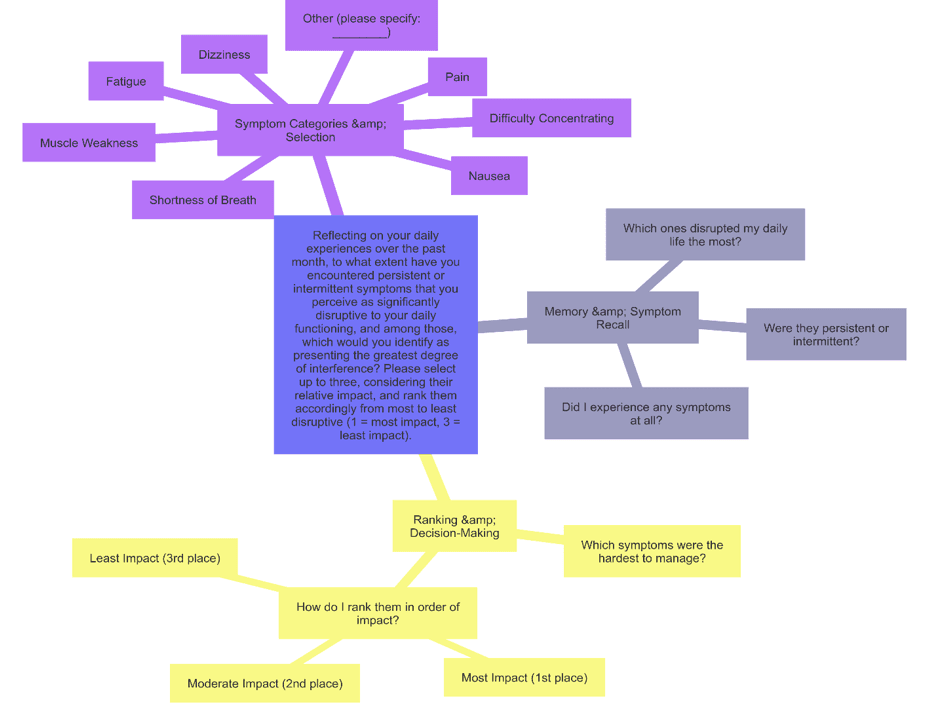
What the Map Shows
Two-step task: first select, then rank. Patients cannot complete the item without doing both stages.
Comparative integration: they must evaluate multiple symptom domains (physical, cognitive and functional) and judge relative impact.
Working memory strain: requires holding multiple symptoms in mind simultaneously whole ordering them by importance.
"Other” option escalates load: adds open recall and writing, plus integration inn to the ranking system.
Cross-domain comparisons: pain versus fatigue versus concentration versus nausea = different modalities, hard to weigh against each other.
CBS Item Type Comparison
Item Type | Example | Core Task | WM Load (chunks) | Why It’s Harder / Easier |
Binary (Yes/No) | “In the past week, did you experience any pain?” | Recall if event occurred → map to Yes/No | ~4–5 | Simple syntax and binary response; but recall and ambiguity of “pain” push against capacity. |
Simple Frequency | “Over the past month, how often have you felt anxious or worried about your health?” | Recall episodes → aggregate → map to ordinal anchor | ~5–6 | Familiar scale, clear timeframe; but 30-day recall, fuzzy anchors, and attribution increase demand. |
Complex Frequency | “…how often… involuntary, distressing mental imagery (nightmares/flashbacks) linked to trauma?” | Recall → classify → attribute to trauma → map to scale | ~6–7 | Clause stacking, paradoxical attribution, emotional salience drive load. |
Global Evaluative | “How would you rate your overall quality of life, considering both physical symptoms and emotional well-being? What factors contribute most?” | Integrate domains → form global judgment → attribution | ~6–9 | Abstract construct + domain integration + stigma. Heavy synthesis burden. |
Checklist (Multi-select) | “Which emotional effects… as a result of your health condition? (Select all that apply)” | Recognition → scan list → attribute each → multi-select | ~6–7 (scales with list length) | Recognition helps, but scanning, overlaps, and multi-response inflate load. |
Descriptor-Based Ordinal | “To what extent do descriptors (aching, stabbing, burning… punishing) align with your pain experience?” | Recognition + scaling for 19 descriptors | 8–10+ sustained | Requires repeated mapping across many overlapping descriptors, scale use, and response mechanics. |
Ranking Task | “In the past month, which of the following symptoms have caused the most difficulty? Select up to three and rank them (1–3).” | Recognition → selection → comparative ranking | ~7–8 | Dual task: choose relevant symptoms and then prioritise. Requires cross-domain comparisons and metacognitive ordering. |
What We Learn
Ranking items occupy a distinct position in the COA CBS landscape:
They are lighter than descriptor-based inventories, which require rating 19 descriptors across multiple dimensions, but heavier than simple checklists because the introduce a comparative layer.
Patients must first select symptoms and then prioritise them. This is a two-step process that creates serial and parallel working memory demands.
The task requires cross-domain comparisons, weighing pain against fatigue or nausea against difficulty concentrating. These are judgements that are subjective, culturally variable and often change over time.
The “other” field introduces additional recall and writing burden, plus the challenge of integrating self-generated content into the ranking.
In CBS terms, ranking tasks force patients into a metacognitive stance: they must not only report symptoms but also reflect on their relative impact. This transforms recognition into prioritisation. This is a qualitatively different form of cognitive burden.
So far, we have examined binary, frequency, checklist, descriptor-based, global and ranking questions. In the next article, we turn to a shared-step frequency item set. This is a matric-style design that is often used in PRO and COA instruments.
Thank you for reading,
Mark Gibson, Leeds, United Kingdom
Nur Ferrant Morales, Ávila, Spain
September 2025
Originally written in
English