
The Cognitive Burden Simulator: Descriptor-based Pain Items
Jan 6, 2026
UK
,
Spain
This article uses the Cognitive Burden Simulator (CBS) to examine the mental load that patients may face when responding to a descriptor-based pain item. It asks:
When considering the nature of any discomfort you may have experienced, to what extent do the following descriptors subjectively align with your personal perception of the pain’s characteristics, intensity, and overall impact on your daily functioning?
Please circle or mark one option for each descriptor.
Response Scale:
0 = Not at all 1 = Slightly 2 = Moderately 3 = Strongly 4 = Extremely
Descriptor | 0 = Not at all | 1 = Slightly | 2 = Moderately | 3 = Strongly | 4 = Extremely |
Aching | ☐ | ☐ | ☐ | ☐ | ☐ |
Stabbing | ☐ | ☐ | ☐ | ☐ | ☐ |
Burning | ☐ | ☐ | ☐ | ☐ | ☐ |
Cramping | ☐ | ☐ | ☐ | ☐ | ☐ |
Crushing | ☐ | ☐ | ☐ | ☐ | ☐ |
Shooting | ☐ | ☐ | ☐ | ☐ | ☐ |
Tingling | ☐ | ☐ | ☐ | ☐ | ☐ |
Radiating | ☐ | ☐ | ☐ | ☐ | ☐ |
Numb | ☐ | ☐ | ☐ | ☐ | ☐ |
Dull | ☐ | ☐ | ☐ | ☐ | ☐ |
Sharp | ☐ | ☐ | ☐ | ☐ | ☐ |
Gnawing | ☐ | ☐ | ☐ | ☐ | ☐ |
Heavy | ☐ | ☐ | ☐ | ☐ | ☐ |
Throbbing | ☐ | ☐ | ☐ | ☐ | ☐ |
Cutting | ☐ | ☐ | ☐ | ☐ | ☐ |
Pressing | ☐ | ☐ | ☐ | ☐ | ☐ |
Exhausting | ☐ | ☐ | ☐ | ☐ | ☐ |
Sickening | ☐ | ☐ | ☐ | ☐ | ☐ |
Punishing | ☐ | ☐ | ☐ | ☐ | ☐ |
Each descriptor is then rated on an ordinal intensity scale (not at all, slightly, moderately, strongly, extremely). This format goes beyond a simple checklist: rather than just ticking descriptors that apply, patients must evaluate the degree of fit between each term and their lived experienced of pain.
This format forces patients to:
1. Scan all 19 descriptors
2. Recall and match each to their pain experience
3. Judge the degree of fit for each descriptor
4. Map to a fuzzy ordinal scale (Not at all to Extremely)
So, that’s recognition + multidimensional evaluation + mapping, repeated 19 times. This is an enormous cognitive and emotional load.
What Makes This Item Easy
It uses a familiar anchor scale
The 0-4 range (Not at all to extremely) is straightforward and many patients will have seen similar Likert-type scales before.
Recognition over recall
Patients do not have to generate descriptors themselves. They are given a menu of terms (aching, stabbing, etc.) to match against their experience. Recognition is less demanding than free recall.
Concrete sensory words
Many descriptors, such as “sharp”, “burning”, “stabbing”, are everyday terms that clearly evoke distinct sensation, which can aid matching.
What Makes This Item Difficult
1. Multiple concepts to juggle.
To answer, patients much hold in mind:
The stem (“Considering discomfort…”)
The response task (mark one option per descriptor)
The ordinal scale (0 = Not at all to 4 = Extremely)
The instruction to apply it to every item (19 times)
The distinction between descriptors (many are overlapping or subtle)
Their personal experience of pain across characteristics, intensity and impact.
This is already 7 active concepts before even starting the first row and the load compounds across 19 repetitions.
2. Scale-task integration
Unlike a checklist (“tick all that apply”), this requires mapping each descriptor to a degree of fit. Patients must decide not only whether a descriptor applies but how strongly.
3. Scanning and fatigue
Nineteen descriptors require sustained attention. Patients must scan the list without skipping lines and remember to mark exactly one response for each. This can lead to “tick-box fatigue”.
4. Overlap and redundancy
Terms like dull, aching, gnawing and throbbing may blue together. Patients may hesitate: “Is my pain dull or aching? Or both?” This overlap can increase uncertainty and slow down processing.
5. Translation problems
In multilingual trials, descriptors often collapse. For example, “aching” and “gnawing” might both be rendered by the same word in another language. “Cramping” and “spasming” may fuse. Patients then face ambiguity and repetition, compounding confusion and cognitive load.
6. Register
The stem is high-register and will – not may – but will serve to alienate many patients.
7. Response mechanics
Patients must remember how to respond (circle or tick one box per row) while working through the list. This step competes for working memory with the semantic judgement.
8. The function dimension is buried in the stem
The stem asks about characteristics, intensity and impact on daily functioning. But the descriptors themselves are mostly sensory (burning, stabbing). Patients may struggle to reconcile these levels of abstraction: “Does ‘exhausting’ mean ‘fatigue’ or ‘pain’? Or it is the pain’s intensity itself?”
Cognitive Load Estimate
Base load (stem, scale, instructions, construct) = 4-5 chunks
Active judgement per descriptor (recognition + mapping + marking) = 2-3 chunks repeated 19 times.
Total demand = easily over 10 chunks sustained, well beyond Cowan’s 4±1 limit, particularly under stress, fatigue or pain.
CBS Insight:
This descriptor-based format looks like simple recognition but in practice it is a hybrid of checklist + ordinal scale + multidimensional integration. Patients must manage not only content (19 descriptors) but also process (scale mapping, response mechanics, scanning). For many, the burden is not just cognitive but also linguistic: translation overlaps and subtle distinctions risk obscuring rather than clarifying the lived experience of pain.
CBS Breakdown Table
Level | Component Type | Text | Notes |
Root | Sentence | When considering the nature of any discomfort you may have experienced, to what extent do the following descriptors subjectively align with your personal perception of the pain’s characteristics, intensity, and overall impact on your daily functioning? | Full stem (long, multi-phrase) |
1 | Frame | When considering the nature of any discomfort you may have experienced | Instructional recall anchor |
1 | Main Clause | To what extent do the following descriptors subjectively align with your personal perception | Core evaluative demand |
2 | Construct | Descriptors | Requires recognition + judgment |
2 | Qualifier | Subjectively align / personal perception | Adds metacognitive layer |
1 | Dimensions | Pain’s characteristics, intensity, impact on daily functioning | Multidimensional judgment scope |
1 | Response Scale | 0 = Not at all → 4 = Extremely | Ordinal mapping required |
1 | Response Format | One mark (circle/tick) per descriptor | Procedural instruction |
1 | Descriptor List (repeated x19) | Aching, stabbing, burning, cramping, crushing, shooting, tingling, radiating, numb, dull, sharp, gnawing, heavy, throbbing, cutting, pressing, exhausting, sickening, punishing | Each requires recognition → mapping → marking |
CBS Visual Map (Conceptual Flow)
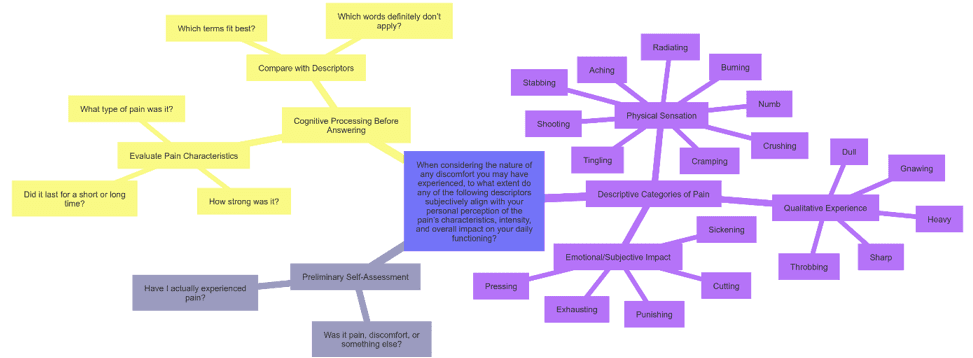
What the Map Shows
Multiple entry points: Before even reaching the descriptors, patients must internalise the stem, dimensions, scale and response format.
Nineteen branches: each descriptor is a separate recognition and mapping task. Even if each feels “simple”, the serial accumulation produces heavy sustained load.
Integration challenge: Patients must balance sensory descriptors (sharp, burning), affective descriptors (sickening, punishing) and functional dimensions (exhausting), all under one framework.
Procedural memory load: Remembering “circle one box per row” competes with semantic processing.
Translation risk: In multilingual use, overlapping or collapsed terms multiply complexity.
Comparison Across types of COA Items
Item Type | Example | Core Task | WM Load (chunks) | Why It’s Harder / Easier |
Binary (Yes/No) | “In the past week, did you experience any pain?” | Recall if event occurred → map to Yes/No | ~4–5 | Simple surface, but recall + ambiguity of “pain” and timeframe fuzziness push against capacity. |
Simple Frequency | “Over the past month, how often have you felt anxious or worried about your health?” | Recall episodes → aggregate → map to ordinal anchor | ~5–6 | Familiar scale and plain words, but 30-day recall, aggregation, fuzzy anchors add complexity. |
Complex Frequency | “Over the past month, how often… involuntary, distressing mental imagery (nightmares/flashbacks) linked to trauma?” | Recall → classify (involuntary, distressing) → attribute → map to scale | ~6–7 | Clause stacking, construct definition, paradoxical attribution, and emotional salience create a heavy load. |
Global Evaluative | “How would you rate your overall quality of life, considering both physical symptoms and emotional well-being? What factors contribute most?” | Integrate domains → form global judgment → causal attribution | ~6–9 | Abstract concept, domain weighing, attribution, stigma. Far beyond Cowan’s 4±1 for many. |
Checklist (Multi-select) | “Which emotional effects… as a result of your health condition? (Select all that apply)” | Recognition → scan list → attribute each → multi-select | ~6–7 (scales with list length) | Recognition easier than recall, but scanning, overlaps, and multi-response inflate load. |
Descriptor-Based Ordinal | “To what extent do descriptors (aching, stabbing, burning… punishing) align with pain experience?” | Recognition + scaling for 19 descriptors | 8–10+ sustained | Requires holding the stem, scale, instructions, and multiple dimensions in mind while repeatedly mapping 19 overlapping terms. Translation issues multiply difficulty. |
What We Learn
Descriptor-based pain items represent one of the heaviest hidden burdens in the COA landscape. On paper, they look like straightforward recognition questions. In practice, they require patients to:
Internalise a long, clause-loaded stem.
Remember the response procedure (circle one option per row).
Recall and evaluate lived experience of pain.
Apply a five-point scale to each of 19 descriptors.
Distinguish between overlapping terms that may collapse in translation.
Sustain this process across a full page of items without fatigue or mechanical responding.
The CBS shows that what seems like a “rich” measure of pain is in fact a hybrid of checklist, frequency and global evaluative demands. Patients are asked to juggle 8–10 concurrent concepts and repeat the cycle nearly twenty times. For many, especially those already coping with fatigue, pain, or stress, this means responses may reflect cognitive endurance and interpretation of language as much as, or more than, the actual quality of their pain.
The next article will focus on a COA item that involves a ranking task, that also looks deceptively simple and creates a qualitatively different cognitive burden compared to the items we have encountered so far.
Thank you for reading,
Mark Gibson, Leeds, United Kingdom
Nur Ferrante Morales, Ávila, Spain
September 2025
Originally written in
English