
The Cognitive Burden Simulator: A Multi-Step Global Evaluation Item (With Follow-Up)
Dec 24, 2025
UK
,
Spain
This article uses to Cognitive Burden Simulator (CBS) model to visualise the cognitive load that an average patient may experience when processing the following multi-step global evaluation item:
“How would you rate your overall quality of life, considering both physical symptoms and emotional well-being? What factors contribute most to this assessment?
Choose from:
· Physical health
· Mental health
· Social support
· Lifestyle.”
What Makes this Item Easy?
1. Familiar concepts
“Quality of life”, “physical health”, “mental health”, “social support” and “lifestyle” are everyday terms most patients will recognise.
2. Explicit guidance
The instruction to consider both physical symptoms and emotional well-being helps anchor the scope, rather than leaving “quality of life” undefined.
3. Structured options for attribution
Patients don’t have to generate factors from scratch; they can choose from a short, clear list of four. Recognition is cognitively easier than free recall.
4. Direct question format
“How would you rate…?” is straightforward, compared to multi-clause, hedged or jargon-heavy stems.
What Makes It Difficult?
1. Abstract global evaluation
“Overall quality of life” is broad and subjective. Patients must synthesise multiple domains into one judgement, which is cognitively taxing.
2. Multi-domain integration
They are explicitly asked to combine physical and emotional dimensions. This requires holding both in working memory and weighing their relative importance.
3. Attributional reasoning
Beyond giving an overall rating, patients have to identify factors contributing most. This involves casual thinking, prioritisati0on and sometimes uncomfortable reflection.
4. Potential conflicts across domains
Patients may struggle if physical health is poor but emotional well-being is strong, or vice versa. Reconciling conflicting signals increases cognitive burden.
5. Social desirability and self-presentation
Some may hesitate to endorse mental health or social support issues due to stigma. This can bias choices and add emotional load.
6. Scale mapping still required
Even with attributional options, the core still involves rating “overall quality of life”. Converting a complex, lived experience into a single category of scale remains difficult.
Summary
This item is “easy” in the sense that its language is familiar and options are limited, making less intimidating than medicalised or jargon-heavy COA questions. However, it is “difficult” because it demands abstraction, integration, prioritisation and causal attribution. These are all high-level cognitive processes.
In practice, patients are juggling at least five concepts at once: overall life quality, physical health, mental health, emotional well-being and the factor list, already exceeding Cowan’s 4±1 working memory limit.
CBS Breakdown Table
Level | Component Type | Text | Notes |
Root | Sentence | How would you rate your overall quality of life, considering both physical symptoms and emotional well-being? What factors contribute most to this assessment? | Full item |
1 | Main Question | How would you rate your overall quality of life | Global evaluation |
2 | Auxiliary Verb | Would | Question framing |
2 | Subject | You | Person answering |
2 | Verb Phrase | Rate your overall quality of life | Predicate |
3 | Verb | Rate | Action required |
3 | Noun Phrase | Your overall quality of life | Object of rating |
4 | Determiner | Your | Defines ownership |
4 | Adjective | Overall | Qualifies "quality of life" |
4 | Noun Phrase | Quality of life | Core construct |
1 | Qualifier (Instruction) | Considering both physical symptoms and emotional well-being | Adds dimensions for integration |
2 | Noun Phrase 1 | Physical symptoms | Dimension 1 |
2 | Noun Phrase 2 | Emotional well-being | Dimension 2 |
1 | Attributional Question | What factors contribute most to this assessment? | Causal reasoning |
2 | Response Options | Physical health / Mental health / Social support / Lifestyle | Attribution categories |
And the CBS Visual Map for this item:
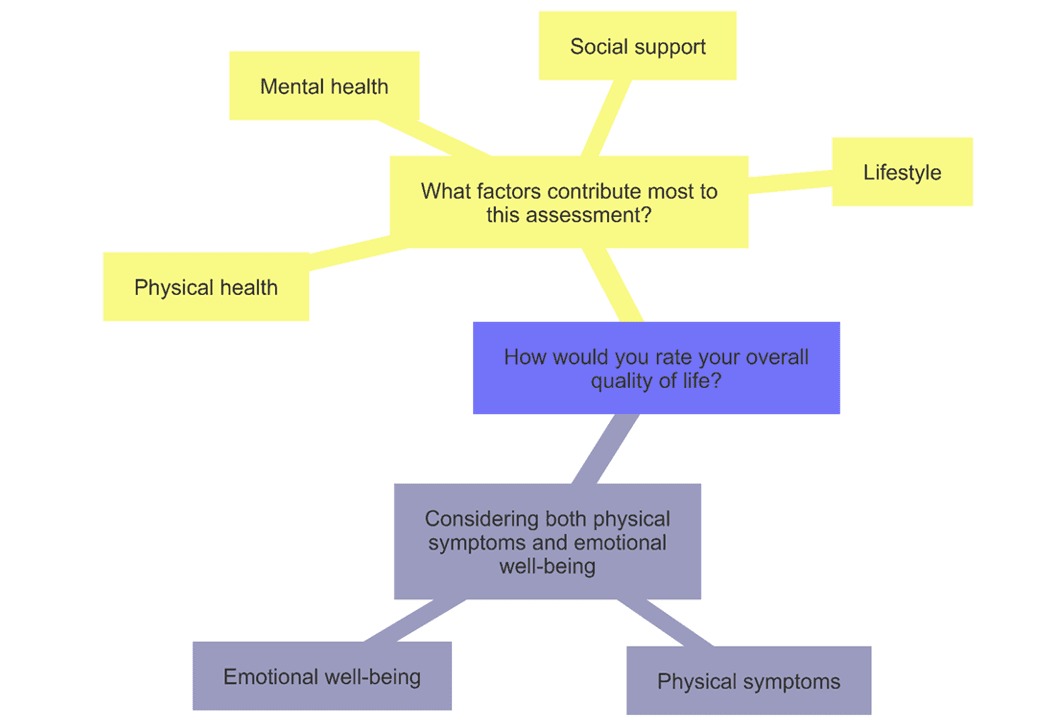
What We Learn
Compared to the simple binary pain item from the previous article, this global quality-of-life item multiplies the processing steps:
Patients must integrate two domains: physical and emotional.
Then make an abstract global evaluation.
Then engage in causal attribution by choosing contributing factors.
Looking at this item through the CBS lens makes clear just how much cognitive work is hidden beneath what looks like a straightforward question. To answer, the patient must first grasp the abstract idea of “overall quality of life”, then integrate two distinct domains (physical and emotional) and finally attribute the cause by selecting factors from a list. That means holding in working memory not only the global judgment but also domain-specific inputs and potential contributors. In practice, this forces the patient to juggle five or more concurrent concepts: a load that already exceeds Cowan’s 4±1 limit for working memory.
What looks like a simple “rating” question is in fat a multi-stage task of evaluation that demands abstraction, integration, prioritisation and attribution. For patients already coping with stress, fatigue or pain, the risk is that the question design itself shapes the answer more than the lived experience it aims to capture.
Side-by-Side Comparisons
Dimension | Binary Item <br> “In the past week, did you experience any pain? (Yes/No)” | Global QoL Item <br> “How would you rate your overall quality of life, considering both physical symptoms and emotional well-being? What factors contribute most?” |
Core task | Recall past week → decide if pain occurred → map to Yes/No | Make an overall judgment of quality of life → integrate physical + emotional domains → identify contributing factors |
Parsing load | Simple structure (one prepositional phrase + one main clause) | Complex structure (main clause + qualifier + attributional clause + factor list) |
Concepts in play | 1. Timeframe (past week) | 1. Overall quality of life |
Working memory demand | ~4–5 chunks → at Cowan’s ceiling | ~6–9 chunks → beyond Cowan, straining Miller |
Response options | Binary (Yes / No) | Rating scale (implicit) + multiple attribution choices |
Sources of difficulty | Ambiguity of “pain” (mild vs severe) | Abstractness of “quality of life” |
Patient experience | Feels “simple” but already requires juggling 4 concepts | Feels familiar in language, but demands abstraction, integration, prioritisation, and attribution all at once |
Notes:
The binary pain item is already cognitively loaded: patients carry around 4–5 concepts just to produce a Yes/No.
The global QoL item adds layers of abstraction, integration, and attribution, forcing patients to juggle 6–9 concepts simultaneously.
This leap pushes the task beyond the natural working memory limits for many patients, especially those under stress, pain, or fatigue.
What looks like a shift from “simple” to “global” is in fact a shift from mental recall to mental synthesis, which is a qualitatively different and heavier burden.
In the next article, we map a frequency-type self-report question to the cognitive processes it demands, from recalling experiences across a defined timeframe, to estimating their occurrence, to mapping that estimate onto fuzzy ordinal scale anchors such as “Sometimes” or “Often”. By breaking this down step-by-step, we can see how a seemingly simple item engages working memory, judgement and interpretation and why this cognitive burden of frequency questions is often underestimated.
Thank you for reading,
Mark Gibson, Harrogate, United Kingdom
Nur Ferrante Morales, Ávila, Spain
September 2025
Originally written in
English